Many of you have asked, “Hey Teenshrink, this is all well and good, but what about teens?” The question is understandable given the name of this blog. But patience, there is method to my madness. In order to make sense of teens, I felt the need to set the stage. Adolescence only really makes sense if you understand the foundation it is built on. Hopefully I have shed some light on this foundation so far.
Teen transitions

Adolescents sit perched on the gateway between childhood and adulthood and it is in these years that an astounding array of mental health difficulties have their origins. Roughly half of all lifetime mental disorders, in most studies, are found to start by the mid-teens and three quarters by the mid-20s. The peak age of onset for all mental illnesses is 14 (according to the National Comorbidity Survey). It may come as little surprise therefore that many parents are overcome by a strange pessimism at the mere thought of parenting their children through these ages. But with some insight into the brain and soul of the teenage years it should be possible to reduce such pessimism.

Eric Ericson was one of the first theorists to extend the theory of development out of childhood. This was unlike Freud and many of his early disciples who seemed to have difficulty looking beyond early childhood. According to Ericson’s theory, basic interpersonal patterns of trust, cooperation, autonomy, mastery and sensitivity to shame and guilt may have been established by the time of adolescence, but the challenges of identity formation and integration into the broader community await the teenage years.
Adolescence has been defined as beginning with the onset of puberty and ending with the establishment of an independent role in society. However that timespan seems to be expanding in our western culture. The average age of puberty has been decreasing (for reasons that have not been established), and the age of establishing an independent role in society has been getting later. With the age of social media upon us, this time period has become ever more complex and tumultuous!
The Teenage Brain

So what is going on in the brain during these years? Although the brain has achieved 90% of its size by the age of 6, the amount of white matter in the brain continues to increase into the thirties. White matter is the part of the brain that acts like highways. Meanwhile the houses in the city of the brain are the gray matter. The gray matter begins to decline through middle adolescence. This has been referred to as synaptic pruning, but occurs inconsistently across various brain regions. The prefrontal cortex is one of the areas that fully matures through this time period. With its increased differentiation and interconnection the teenager becomes able to think more abstractly and experience greater self-awareness than ever before. This leads the adolescent to begin to ask him or herself the question “Who am I and where do I fit in?” in ways that younger children cannot yet do. The answer to this question for us, among the most social of mammals, has been incredibly important to our survival.
The Social Brain

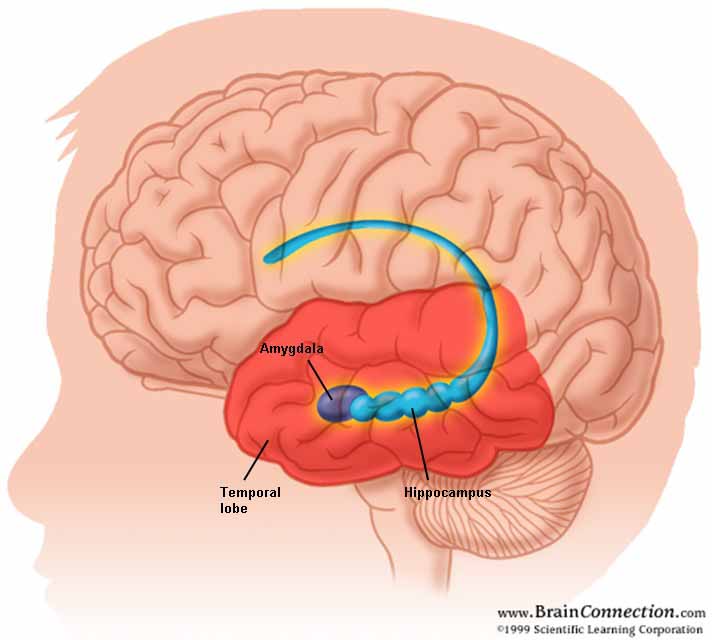
Perhaps for this reason the teenage brain appears to demonstrate a heightened sensitivity to social stimuli such as facial expressions. The medial frontal area of the prefrontal cortex used by adolescents to decode facial expressions is more actively linked to the emotional brain than the superior temporal area used by adults for similar tasks . Therefore, the job of decoding facial expressions is much more tightly linked to the emotional brain in adolescence than it is in adulthood. For this reason it seems that non-verbal signals are more likely to lead to powerful physical and emotional reactions in adolescence than at any other time of life.
Male and female development, of course, take somewhat different trajectories. Male development in adolescence is associated with increases in the hormones testosterone and vasopressin, which act synergistically and result in increased intermale competition, while female development is associated with increased estrogen and oxytocin, which result in an increased tendency towards female relational bonding, which as we know can result in painful exclusion when it goes awry. (See Panksepp's "Archeology of Mind")
Of Peers and Parents

Strangely as a culture it seems we in the “western developed world” have gone down a rather strange road when it comes to how we approach this critical time of adolescence. In their book "Escaping the Endless Adolescence", psychologists Joseph and Claudia Worrell Allen note that teenagers in the US spend just 16 hours per week interacting with adults and 60 hours with other adolescents. One century ago it was almost exactly the opposite, as it continues to be in more traditional societies. The implications of this may be very significant.

Gordon Neufeld and Gabor Mate argue convincingly in their book, "Hang Onto Your Kids", that this environment, devoid of adult influence, increases the pressure on peer relationships and interferes with the parent child attachment bond that remains an important tether for the ongoing development for the adolescent. With weaker parent-youth bonds, youth are more likely to turn to their much more available same aged peers to meet their ongoing needs for nurturance and guidance. With the increased power of technology and social media this becomes seductively easier, and many parents unwittingly encourage this. Unfortunately, the results for the parent-teen relationship can be devastating. Once teens have tuned out parent for their nurturance needs, and tuned in their same aged peers, parents lose their natural parental authority and peers take over this powerful mantle of influence. The guidance these teens tend to receive from other adolescents rarely encourages the long term goals and values that adult caregivers would be likely to encourage. This shift in focus to same aged relationships is something that is almost taken for granted in our culture, but it inevitably leads to frustration among parents who find their offspring beyond their influence. Often parents either throw up their hands in defeat, or alternatively turn to harsh punishments which can result in further estrangement and resentment and breakdown of trust.
The Rising Tide

As adolescence proceeds, we see an increase in the incidence of depression, suicidal ideation, substance misuse, eating disorders and psychosis. Families and children face many pressures, such as illness, divorce, financial and personal upheaval which can accumulate and place strain on parent child bonds. With few alternate adults to turn to, youth often turn to their same age peers during these challenges, for a time often coming across as carefree and unaffected. However the world of peer relationships is unstable, many peers are struggling with their own problems, and hostility and rejection are everywhere to be found. As these pressures accumulate and as peers turn to one another, or turn inward, the chances of mental health issues reaching critical levels increases steadily. Drugs, self harm and disordered eating can serve as powerful ways to avoid pain and modify stress in the short term, but can quickly turn into compulsive patterns that are difficult to change, complicating long term social problems. Suicide looms as an ultimate "way out" that all too many youth consider. As parents find their influence on their troubled teens waning, their frustration and stress level naturally rise, and parents are themselves often under-supported in this world of ever decreasing social capital. (See Putnam "Bowling Alone")
Turning the Tide
Hopefully, with our greater understanding of neurobiology and of the developmental importance of the attachment relationship, we as a society may come to rethink our approaches to our vulnerable youth. Rethinking our approach to isolating youth in same age cohorts and instead integrating adolescents more successfully into integrated, age stratified, social contexts would certainly be worth considering. Perhaps by doing so we may see some reduction in the rates of adolescent mental health problems, violence, substance abuse and relationship problems that have come to dominate our news sources in recent years.